Calculations for Analyzing Inspection Results
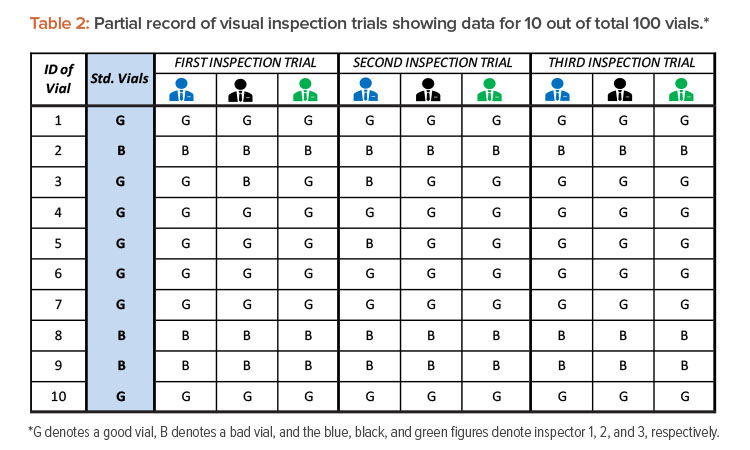
After completing three visual inspection trials by three inspectors and recording observations in Table 2, the following data are used to begin outcomes analysis:
- Total number of inspections = Total number of vials inspected (100) × Number of inspection trials (3) × Number of inspectors (3) = 100 × 3 × 3 = 900 total inspections
- Total number of good vials inspected = Number of good vials (80) × Number of inspection trials (3) × Number of inspectors (3) = 80 × 3 × 3 = 720 good vials inspected
- Total number of bad vials inspected = Number of bad vials (20) × Number of inspection trials (180) × Number of inspectors (30) = 20 × 3 × 3 = 180 bad vials inspected
From those data, several calculations are run. These calculations and the results are shown in Table 3.
Table 3: Equations, values, and results for calculations.
| Calculation |
Equation |
Values |
% |
| Overall accuracy |
(TotalnumberofinspectionsthatmatchthestandardsTotalnumberofinspections) x 100 |
(862900) x 100 |
95.8 |
| Overall error rate |
(TotalnumberofinspectionsthatdonotmatchthestandardsTotalnumberofinspections) x 100 |
(38900) x 100 |
4.2 |
| Good units rated as bad |
(TotalnumberofgoodunitsratedasbadTotalnumberofgoodunitsinspected) x 100 |
(33720) x 100 |
4.6 |
| Bad units rated as good |
(TotalnumberofbadunitsratedasgoodTotalnumberofbadunitsinspected) x 100 |
(5180) x 100 |
2.8 |
| Inspector accuracy rate |
(NumberofcorrectmatchesbytheinspectorNumberofinspectionsdonebytheinspector) x 100 |
|
|
| Example for inspector 1 |
(280300) x 100 |
93.3 |
| Unit-specific error rate |
(NumberofincorrentmatchesonthespecificunitNumberofinspectionsdoneonthespecifcunit) x 100 |
|
|
| Example for vial 11 |
(89) x 100 |
88.9 |
| Good units rated as bad by inspector |
(NumberofgoodunitsratedasbadbytheinspectorNumberofgoodunitsinspectedbytheinspector) x 100 |
|
|
| Example for inspector 1 |
(17240) x 100 |
7.1 |
Using these calculations, we can then determine upper and lower bound CIs for inspector accuracy rates on good units with a 95% CI (α = 0.05):
Lower bound value = 11+n−x+1xF2(x+1),2x,α/2
Upper bound value =x+1n−xF2(x+1),2x,α/21+x+1n−xF2(x+1),2x,α/2
where
x = number of correct matches with good units by the inspector
n = total number of good units inspected by the inspector
Fv1,v2,α= F distribution table value with v1 and v2 degrees of freedom at alpha (95%) level of confidence
Example for inspector 1:
Lower bound value = (11+240−223+1223F2(240−223+1),(2x223),0.05/2)x100
= 88.9%
Upper bound value =(223+1240−223F2(223+1),2(240−223),0.05/21+223+1240−223F2(223+1),2(240−223),0.05/2)x100
= 95.8%
Note: It is best to use statistical software to calculate the exact CI because the formulas are complex. For manual calculation, a relatively simple normal approximation method can be used. The formulas are as follows:
formula (p±Z1−(α/2√p(1−p)n)x100
where
P=NumberofcorrectmatcheswithgoodunitsbytheinspectorTotalnumberofgoodunitsinspectedbytheinspector
Z1-(α/2)=1.96 for 95% CI
n = total number of good units inspected by the inspector
Graphical Tools to Interpret Trial Data
The data obtained from inspection trials can be graphically illustrated by using a spreadsheet application or commercially available statistical software.
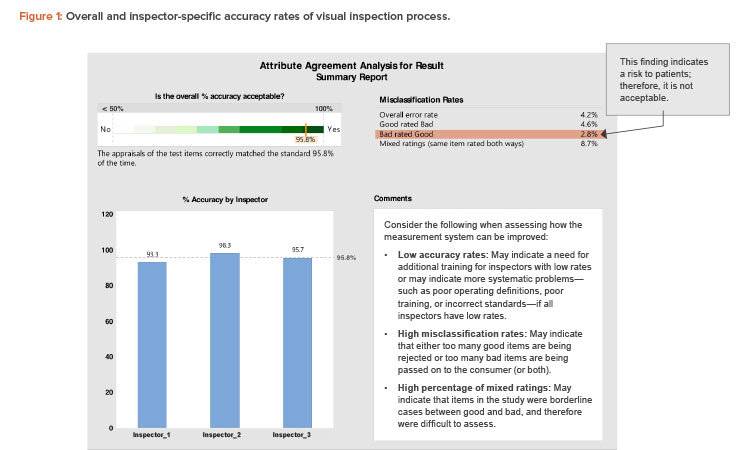
The first report (Figure 1) shows the overall accuracy of the visual inspection process (95.8%). The overall process complies with the minimum acceptance for accuracy of 95% (a justifiable limit).
Figure 1 also compares the individual accuracy of the three inspectors. Inspector 1 had an accuracy rate of 93.3%, which is below the acceptance accuracy limit. Hence, inspector 1 needs to be retrained.
A point of concern related to the “misclassification rate” in Figure 1 is the presence of defective units rated as good units (bad rated good). Units misclassified as good may cause health risks to patients and are therefore unacceptable from the GMP perspective. The misclassifications might have been due to a specific inspector’s errors, or they might be borderline cases for which it is difficult for any inspector to differentiate between good and bad units.
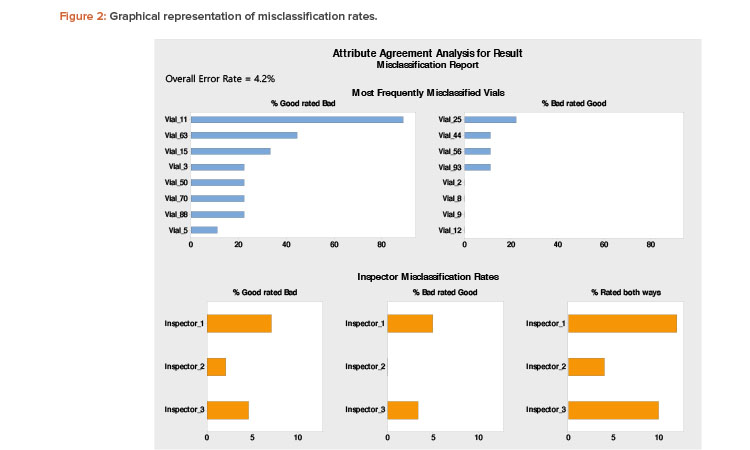
Figure 2 can be useful to interpret misclassification rates. A low rate of accuracy overall and across all inspectors indicates the need to improve the effectiveness of visual inspection procedures, arrangements, or training.